Early pregnancy care resides at the intersection of rapid diagnosis, complex counselling, and long-term psychological impact. While a critical window of development, ectopic pregnancy remains a leading cause of maternal morbidity—occurring in 1% to 2% of pregnancies and accounting for nearly 6% of pregnancy-related deaths. As global caesarean rates rise, the increasing incidence of caesarean scar pregnancies (occurring in roughly 1 in 2,000 gestations) requires us to re-evaluate their role within the placenta accreta spectrum. This month, we bridge clinical learning with compassionate practice, examining diagnostic pitfalls, CTG monitoring in high-risk multiples, and the vital management of psychological sequelae following loss.
WEEK 1 • CTG
The "Disappearing" Membrane
Presented by Zoe Slack
BACKGROUND
31-week MCDA scan: intertwin membrane difficult to see and free-floating, raising concern for septostomy.
INTERPRETATION
Septostomy effectively converts MCDA twins into a single-sac pregnancy with much higher cord-entanglement risk; any "disappearing" membrane should trigger senior review and closer surveillance.
OUTCOME
At 34 weeks, SROM was followed by membrane entanglement around one twin’s leg causing transient ischaemia; both babies were delivered safely by caesarean.
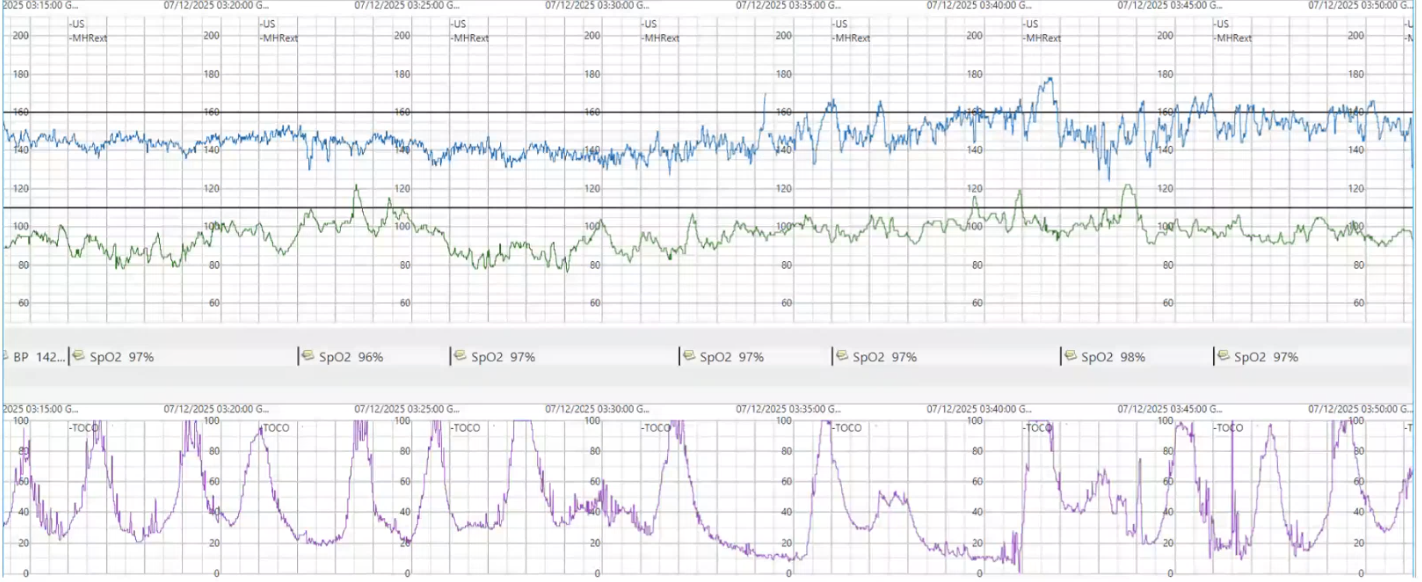
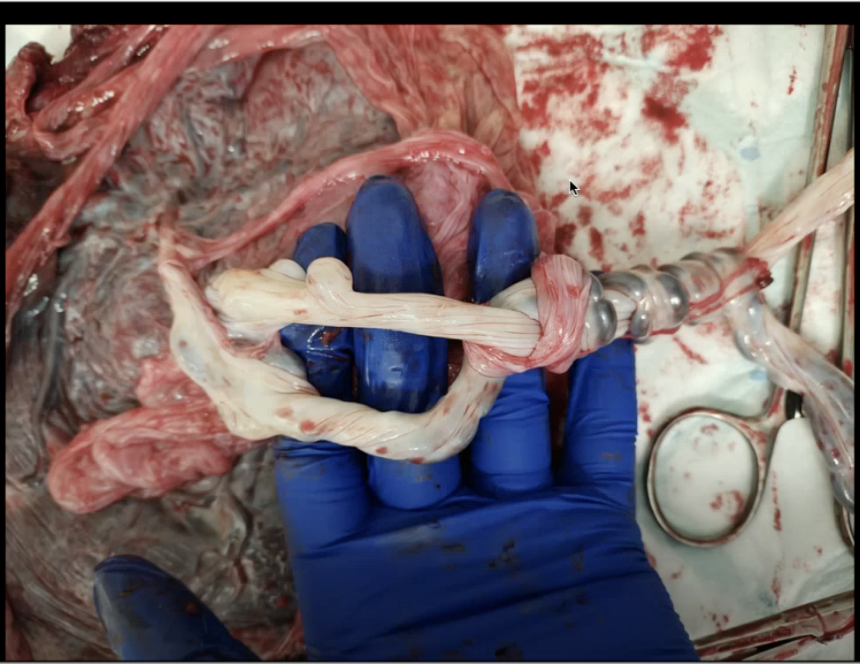
💡 CLINICAL PEARLA disappearing membrane is a high-risk red flag. This image (Fig. 2) shows the physical cause of the foetal distress: the ruptured membrane allowed one cord to wrap around the other four times. This entanglement, tightened by membrane debris, caused both cords to be compressed simultaneously during uterine activity, preventing the twins from tolerating contractions.
Figure 1. CTG trace showing acute foetal distress during labour.
Figure 2. Placental cord and membrane entanglement.
WEEK 2 • GYNAE JC
Posttraumatic stress, anxiety and depression following miscarriage and ectopic pregnancy: a multicentre, prospective cohort study
Am J Obstet Gynecol, 2019•Presented by Shehani Alwis
KEY FINDINGS
Large multicentre cohort of women after miscarriage, ectopic pregnancy, molar pregnancy and PUL followed at 1, 3 and 9 months with validated PTSD, anxiety and depression scales.
KEY RESULTS
High rates of PTSD, anxiety and depression shortly after early pregnancy loss, with a substantial minority still symptomatic at 9 months; many women declined participation because they did not want to be reminded, highlighting classic PTSD avoidance.
TAKE HOME
Do not assume emotional recovery tracks physical recovery: normalise talking about PTSD, anxiety and depression after early loss and build signposting to psychological support into routine follow-up.
Caesarean Scar Pregnancy Spectrum: Standardised Classification and Terminology
J Ultrasound Med, 2026•Presented by Lucy Thorn
KEY FINDINGS
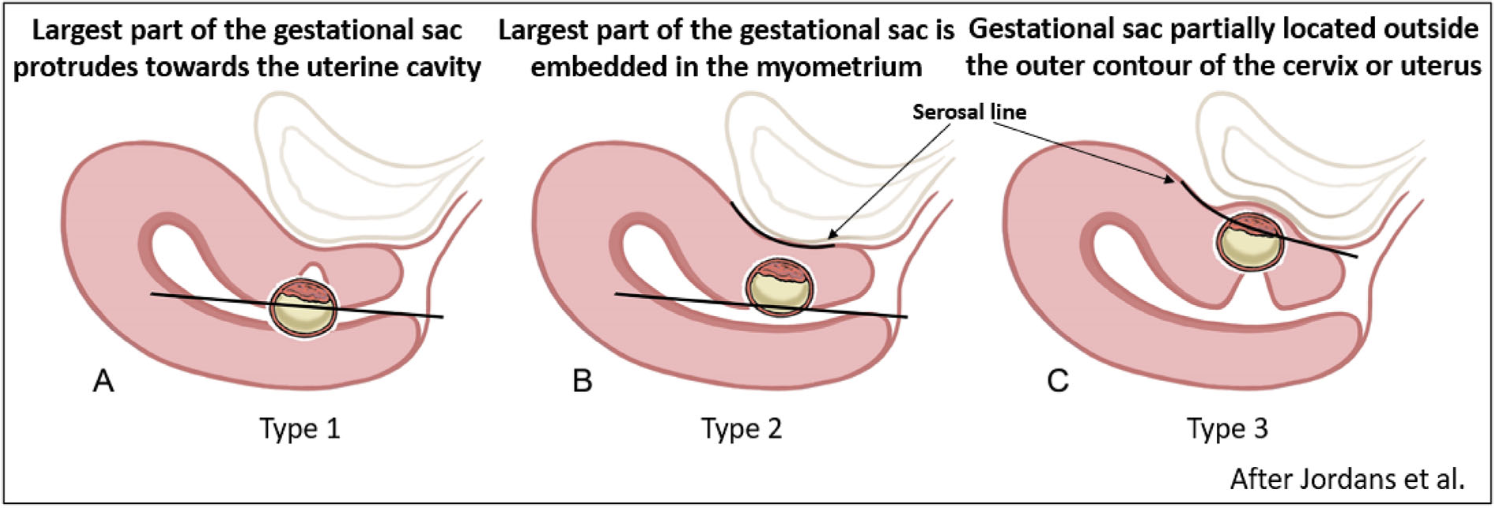
CSP is increasingly seen with rising caesarean rates and sits on the same spectrum as placenta accreta spectrum (PAS). This paper proposes a three-type system based on where the sac sits relative to the scar and cavity.
KEY RESULTS
Type 1 – on the scar, mostly in the cavity: best chance of reaching term.
Type 2 – in the niche: high risk of PAS.
Type 3 – exogenous, bulging towards the bladder: highest risk of rupture and major haemorrhage.
TAKE HOME
Classifying CSP as type 1–3 at first-trimester scan helps stratify risk, support shared decision-making and plan follow-up in centres experienced with PAS before catastrophic bleeding occurs.
Figure 3. Definition and sonographic reporting system for caesarean scar pregnancy in early gestation: the modified Delphi method
Before the era of simple plastic dipsticks, clinicians relied on the Hogben test. To confirm a pregnancy, a woman's urine was injected into an African clawed frog; if the pregnancy hormone hCG was present, the frog would ovulate and lay eggs within 24 hours. When modern chemical tests arrived in the 1960s, these "living lab tests" were no longer needed. Thousands were released into the wild, inadvertently spreading a deadly fungus (chytrid) that has since caused devastating population declines and extinctions of amphibians worldwide. It is a sobering reminder that our instant diagnostic tools are built on decades of animal-based science—and a global ecological footprint.